Low-level laser therapy (LLLT) has gained significant popularity and praise over the past decade for its safe and effective pain relieving functions, as it has become integrated into medical clinics worldwide, and used on tens of thousands of satisfied patients.
As such, there is much curiosity from a variety of health professionals, doctors and allied health workers about the mechanism of action behind low-level lasers, as well as the most versatile laser on the market, the EVRL by Erchonia. As more medical clinics continue to search for treatment options that yield the greatest results, comfort and ease for their patients (as well as ease of use for the clinics themselves), here’s a look into the scientific mechanisms behind the EVRL laser, including their clinical applications and notable differences compared to other LLLT devices currently available on the market.
This is an educational summary, originally presented in webinar form by Sports & Exercise Chiropractor, Brett Jarosz, who has a special interest in clinical neuroscience and rehabilitation. You can access a free recording of the webinar here.
Low Level Laser Therapy: Where Has It Come From?
To give you a bit of background on how low-level laser was first introduced into the market and has since evolved, it first presented back in the early 1960’s, as two devices called the Ruby laser and the Helium-Neon (HeNe) laser. The first glimpse into the broad scope of the laser’s potential effects came in 1967, when Hungarian physician, Endre Mester, hypothesised that if the laser was used on a mouse, the light radiation would lead to cancer – and tested his theory.
The findings were profoundly unexpected. First, he found that applying laser light to the backs of shaven mice actually induced their shaved hair to grow back at a much faster rate than the unshaven mouse. Next, he demonstrated that laser could also stimulate wound healing in mice. These results were soon tested on human patients with non-healing skin ulcers, producing the same beneficial results – accelerated healing, cellular growth and proliferation, and significant improvements to a person’s health circumstances surrounding the ulcer.
It is these findings that formed the foundations for LLLT to be studied and developed over many decades into a highly effective therapeutic procedure that is used in three main ways [1, 2]:
- To reduce inflammation, edema, and chronic joint disorders
- To promote healing of wounds, deeper tissues, and nerves
- To treat neurological disorders and pain
Over the past decades, LLLT has been extensively studied in various clinical settings and applications, and across a wide range of medical professions. Over 100 randomised controlled trials with positive outcomes have been published [3] for the use of LLLT in osteoarthritis, tendinopathies, wounds, back pain, neck and shoulder pain, post surgical pain, heel pain, fungal nail infections (onychomycosis), acne, muscle fatigue, peripheral nerve injuries, strokes and body sculpting. Over 500 placebo-controlled trials with positive outcomes have also been published.
Alongside the promising outcomes in trials for LLLT, the FDA have cleared Erchonia’s EVRL low-level laser to be used safely and effectively on back pain, neck and shoulder pain, post surgical pain, heel pain, fungal nail infections, acne and body sculpting – the most FDA clearances of any LLLT device – making it a very trusted and reputable treatment for patients and clinicians alike.
Low Level Laser Therapy: What Is It?
LLLT is described as “low level” because of its use of light energy at densities that are low. Unlike many other medical lasers, LLLT does not have an ablative or thermal mechanism, but instead works via a photochemical effect. To best understand how this works, think of the process of photosynthesis in plants: the light from the sun is absorbed by the plant and it exerts a chemical exchange. This is very similar to the process in humans when exposed to laser light, although we have our own particular molecular chromophores that absorb certain types of wavelengths of light to induce a specific photochemical effect.
As we start to further describe the mechanism of action LLLT and how it produces its effects, it is important to note that the light source (whether it be a laser, an LED or infrared) and the dosage (measured in joules per cm2) is particularly important to make note of, as there is an optimal dose of light for any particular application, and doses higher or lower than this optimal value may have either no therapeutic effect – or a detrimental effect. Our focus on the benefits and mechanism of action of LLLT, which is characterised by a biphasic dose response, is able to be produced because lower doses of light are often more beneficial than high doses. [4, 5, 6]
Laser Classes: What Are They And Where Does LLLT Sit?
Having different lasers presented alongside their laser classes is often a point of confusion. As an overview, there are four basic classes of laser, and they’re classified for safety purposes, according only to their potential for causing injury to the eyes and skin of humans.
Simply put, both Class I and II lasers are relatively safe for eye (and skin) exposure, as our human blink response (and our eyes’ light aversion response) offers enough protection from any harmful effects of the light, simply through blinking. Class III and IV lasers, on the other hand, are considered hazardous, as they are powerful enough to cause eye damage in a time shorter than either the human blink reflex can offset, or the human blink reflex is bypassed due to the nature and invisibility of the beams, like in the case of infrared. To get into the specifics [7]:
- Class 1 and 1M lasers are safe under reasonably foreseeable conditions of operation. Class 1C lasers are used in medical and cosmetic applications. The laser is only applied when the emission port (aperture) is in contact with target tissue such as skin.
- Class 2 and 2M lasers emit visible light at higher levels than Class 1, but eye protection is provided by aversion responses such as the human blink reflex.
- Class 3R lasers produce visible and invisible light that is hazardous under direct viewing conditions. There is low risk for eye injury provided the exposure time is short. There is no risk for skin injury.
- Class 3B lasers produce visible or invisible light that is hazardous under direct viewing conditions; either they are powerful enough to cause eye damage in a time shorter than the human blink reflex (0.25 seconds) or the blink reflex is by-passed due to the invisibility of the beam. Laser products with power output near the upper range of Class 3B may also cause skin burns.
- Class 4 lasers are high power devices capable of causing both eye and skin burns, their diffuse reflections may also be hazardous and the beam may constitute a fire hazard.
Erchonia’s EVRL laser is strictly a class 2 laser, meaning that it poses no risk of injury to the eyes or skin, as offset by our regular blinking reflex.
Low Level Laser Therapy: Mechanism Of Action
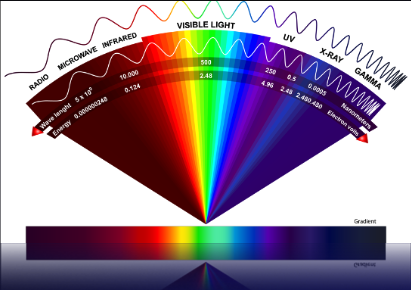
To better understand how LLLT works, it’s important to understand the laws and principles of photobiology [8]. The first law states that for low power visible light (which is in the 400nm to 700nm wavelength spectrum, red to violet coloured light) to have any effect on a living biological system, the photons produced by the laser must be absorbed by some molecular photoreceptors, or chromophores. A chromophore is a part of a molecule that imparts a predetermined colour to the compound of which it is an ingredient – meaning that it’s responsible for its colour. Examples of chromophores can be seen in chlorophyll, haemoglobin, and cytochrome c-oxidase (CcO) within your mitochondria. It is actually this CcO photoreceptor that absorbs and responds to the 635nm light wavelength (and its photons) emitted by the EVRL laser to produce physiological changes.
Next, it’s important to know that any photons that are delivered into living tissue can either be absorbed or scattered [9]. Scattered photons will eventually be absorbed or will escape from the tissue in the form of diffuse reflection. For laser therapy to be able to produce therapeutic effects, we need the light to be absorbed, as when scattered photons escape from the tissue in the form of diffuse reflection, they cannot be of therapeutic value.
It’s also important to understand the concept of energy in terms of light therapy, and the difference between energy and power. “Energy” refers to the photonic energy that a specific laser wavelength is imparting. “Power” only refers to the actual units of a laser – e.g. a 40 Watt laser or a 7.5 milliWatt laser. As it relates to laser therapy, however, it is the energy unit that is most important and related to the therapeutic effects of a laser and its safety profile, with the energy produced by a dose of light from a laser depending only on the number of photons and on their wavelength (identified by their associated light colour). As illustrated in the image below, blue photons have more energy than green photons, that have more energy than red photons, and so on.
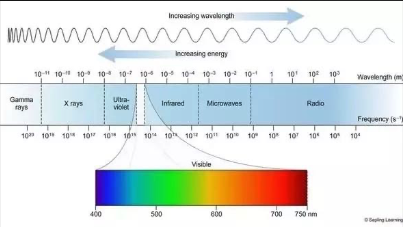
Looking at this chart above, the absorption and scattering of light in tissue are both much higher in the blue region of the spectrum than the red, as the tissue scattering of light is always higher at shorter wavelengths. This means that the laser wavelength emitted by the EVRL – a red 635 nm wavelength, has much higher absorption and much less scattering – meaning many more of the photons are being used to produce a therapeutic effect, as opposed to being lost in diffuse reflection.
All of these factors, paired with the fact that red wavelengths are primarily absorbed by the CcO within the mitochondria (to then go on to produce a therapeutic effect), sheds important light on exactly how the EVRL laser is able to target the cells and produce the beneficial effects that it does.
What effects does LLLT have on the mitochondria?
Being the “powerhouse” of your cells and where energy is produced, having the CcO within the mitochondria effectively absorb the monochromatic red visible light by components of the cellular respiratory chain have shown to produce effects including:
- Increased proton electrochemical potential
- More ATP synthesis
- Increased RNA and protein synthesis
- Increases in oxygen consumption, membrane potential, and enhanced synthesis of NADH and ATP
- Ultimately, this means that the absorption of the light wavelengths produced by the laser leads to the increased production of ATP and cellular energy.
Nitric oxide (NO) photodissociation is another important effect of LLLT. Nitric oxide is produced in the mitochondria, and can inhibit cellular respiration by binding to both iron and the CcO photoreceptor, and competitively displacing the oxygen that is needed by our cells for effective function and energy production. So what laser therapy also does is photodissociates the NO from the CcO, thereby allowing an immediate influx of oxygen and the resumption of mitochondrial respiration and the generation of reactive oxygen species. These reactive oxygen species then create the gene transcription, meaning it produces an overall shift in favour of greater oxygen oxidation, part of which is the stimulation of NF Kappa B, which is the cause of gene transcription of protective and stimulatory gene effects.
Summary: the red wavelength produced by LLLT is absorbed by the CcO photoreceptor, resulting in that light dissociating nitrogen oxide, which allows more oxygen to be able to come in and bind within the mitochondria. This allows appropriate cellular respiration, ATP energy production, and an improvement in the reactive oxygen species, and through this process we get an enhancement in protective and stimulatory gene products.
The effects of the downstream cellular response
As a result of the effects mentioned above, we also get some downstream cellular responses, with clinical studies having indicated that at low doses, LLLT can prevent cell apoptosis and improve cell proliferation in several types of cells including fibroblasts, endothelial cells and lymphocytes, as well as improve cell migration and adhesion. This means it has a direct response on areas such tissue healing and immune response, giving further insight into how the laser can produce the beneficial effects that it does across several therapeutic areas.
Taking this further, we also get the downstream tissue responses to the processes mentioned above. There have been a large number of both animal models and clinical studies that demonstrated highly beneficial LLLT effects on a variety of diseases and injuries, in both chronic and acute conditions. These effects occur as a result of the photochemical effects of LLLT on the cells, and include:
- Enhanced neovascularisation, promoting angiogenesis and increasing collagen synthesis to promote healing of acute and chronic wounds
- Accelerated cutaneous wound healing in rats with a biphasic dose response favouring lower doses
- Stimulated healing of deeper structures such as nerves, tendons, cartilage, bones and even internal organs
- Reduced pain, inflammation and swelling caused by injuries, degenerative diseases or autoimmune diseases
- Mitigated damage after strokes, after traumatic brain injury and after spinal cord injury
Biphasic Dose Response in LLLT
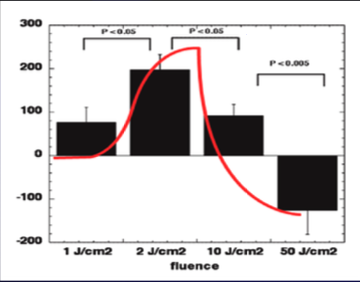
When understanding the mechanism of action of LLLT, it’s also important to talk about the biphasic dose response. A biphasic response has been demonstrated many times in LLLT research and the “Arndt-Schulz Law” is frequently quoted as a suitable model to describe dose dependent effects of LLLT [10]. The ‘Arndt-Schulz law’ states that weak stimuli slightly accelerate vital activity, stronger stimuli raise it further, and eventually, an optimal peak will be reached. However, when an even stronger dose is administered, it will actually start to suppress the response and we can ultimately get a negative response being achieved. The modern term for this occurrence is “hormesis”.
Pictured below is an example of hormesis, or the Arndt-Schultz law, from a low level laser therapy study. In this study, along the x-axis on the bottom of the graph, we can see the amount of joules per centimetre squared emitted. At between 3-5 j/cm2, we can see the most optimal photochemical energy therapeutic effects being delivered. Once we go beyond this to 10 j/cm2, we start seeing a rapid decline in the therapeutic effects, and at the 20-50j/cm2 mark, negative detrimental effects are seen that go beneath the baseline. To better understand this, there are three possible outcomes depending on the dose emitted:
- It suggests that if insufficient energy is applied there will be no response (because the minimum threshold has not been met)
- If more energy is applied, then a threshold is crossed and biostimulation is achieved
- But when too much energy is applied then the stimulation disappears and is replaced by bio-inhibition instead
EVRL Laser: Introduction
The EVRL laser is the most popular handheld pain-relieving laser device worldwide, offering the versatility of both the red and violet therapeutic wavelengths, administered at low levels of maximum to maximise absorption in the mitochondria and the delivery of its therapeutic effects.
It is created by parent company Erchonia, which since their foundation in 1996, has remained committed to furthering the advancement of low-level laser therapy, allowing them to become the leader in this field and offering several LLLT devices with varying therapeutic applications – including the Lunula laser that has revolutionised and optimised the treatment of onychomycosis by podiatrists. Through scientific and clinical studies, there are 25 different FDA indications for LLLT, and Erchonia owns 20 of those indications.
When it comes to the EVRL laser, it works by generating two different wavelengths of light:
- Red 635 nm wavelength at 7.5 milliWatt
- Violet 405 nm wavelength at <5 milliWatt
While we’ve extensively discussed the effects of the red 635 nm laser, it is by combining these two specific wavelengths into one treatment modality that patients are now achieving even better results during clinical studies than just using the 635 nanometer laser alone [11].
The history in combining the two laser wavelengths is that the 635 nm (red) laser was already FDA cleared for pain relief after a study [12] showed significant reductions in pain for LLLT-treated subjects compared to LED sham-treated subjects through the use of the 635 nm wavelength alone. The results of this study were so promising, that the FDA required the study to be repeated – which it was, with identical results. A few years later, Erchonia combined the same 635 nm red laser with the 405 nm violet laser for the same problem as the original study – chronic neck and shoulder pain – to find that even after a single treatment, at 24 hours later, the results outperformed the results achieved with the FDA-approved red (635 nm) laser with regards to the improvement in pain as well as improvement in the range of motion in the shoulder [13]. Hence, the two wavelengths were combined into a single handheld device and the application and popularity of the EVRL laser skyrocketed.
When it comes to pain treatments, of the 15 low level laser FDA indications for pain available, Erchonia has invested into the research and conducted the studies for 9 of these, solidifying them – and their devices – as truly the world leaders in laser for pain relief.
What Is The Difference Between Laser, Infrared & LEDs?
This is a great question – and one that often causes much confusion when looking into laser as a valid, safe and effective form of treatment. The first thing to note is that while having very different wavelengths, mechanisms of action and therefore therapeutic benefits, all three terms are classed under “photobiomodulation” in the therapeutic field, given the official definition of photobiomodulation as “a form of light therapy that utilises non-ionising forms of light sources, including lasers, LEDs, and broadband light, in the visible and infrared spectrum”.
The next key step to helping us understand these three forms of light is better understanding wavelength and energy. Photon energy is measured in electron volts (eV), and the shorter the wavelength, the higher the eV. The longer the wavelength, the lower the eV, as illustrated below:
- 405nm = 3.06 eV
- 532nm = 2.33 eV
- 635nm = 1.95 eV
- 830nm = 1.49 eV
This means that, as an example, the 405 nm wavelength has 70% more energy per photon than 830 nm wavelength. Alongside this, each of the wavelengths (and their associated colours) will have varying depths of penetration into water. With the human body being made of upwards of 70% of water, it’s important to remember that water doesn’t absorb in the wavelength of visible light, which is between ~400-700 nm. This is as the visible light spectrum is too energetic for the vibrations of the water molecule, which is the wavelengths used by the EVRL laser. But the infrared light spectrum, on the other hand, exhibits strong absorptions from vibrations of the water molecule. The result of this infrared absorption is the heating of the tissue since it increases molecular vibrational activity, hence its photothermal effect.
Simply put, visible light penetrates to produce photochemical changes and effects, whereas infrared light is absorbed by water, leading only to physical changes such as the heating effect – making low level lasers and infrared have very different effects and mechanisms of action.
Circling back to the confusion that having lasers, infrared and LEDs all classed under photobiomodulation creates, is that it provides misleading results when looking at studies – if you don’t take the time or have the background knowledge to look deeper below the surface. Specifically, a few years ago in 2020, there was a systematic review published (at the highest level of evidence in research) that concluded that photobiomodulation therapy does not help people with non-specific low back pain from their review of 12 randomised controlled studies [14].
Looking at this study more closely, we see that the lasers used across these 12 included studies had wavelengths of 808nm, 810nm, 828nm, 830nm, 850nm, 904nm and 1064nm – which are all infrared wavelengths and not the therapeutic wavelengths used by EVRL LLLT – meaning that it doesn’t actually clinically encompass photobiomodulation therapy – just the application of infrared wavelengths in this case.
Photochemical vs Photothermal
Focusing in on the difference between lasers and infrared means understanding photochemistry. Specifically, that photochemistry deals with chemical reactions which occur by the absorption of light waves (photons of energy). Photons should contain a sufficient amount of energy to raise molecules to an excited state. When a molecule absorbs a photon of light, it becomes electronically excited. This electronic excitation can result in breaking, reforming, and thus rearrangement of chemical bonds, as well as electron and energy transfer between various parts of a chemical system. You cannot achieve this with infrared light – because instead of penetrating, it’s being absorbed by the water to produce those physical photothermal effects. And with infrared, the eV that it has, doesn’t have enough energy to create a photochemical effect.
Power vs Energy
When we talk about power, we’re talking about the wattage. By adding power to a laser or LED, more photons will be emitted (meaning more buckets of the same wavelength being produced) – but changing power does not change the energy (measured in eV) of the photon. This means that increasing power does not increase the depth of penetration.
Coherence vs Non-coherence
Light is coherent when all of the photons emitted from any light source are travelling in the same direction. As illustrated below, a light bulb produces light that travels in all directions, it’s non-monochromatic – meaning that it’s not the same single colour (like all at 635nm, insead with white light you’ve got 405nm, 605 nm etc coming out), and it’s not coherent, so not all travelling in the same direction.
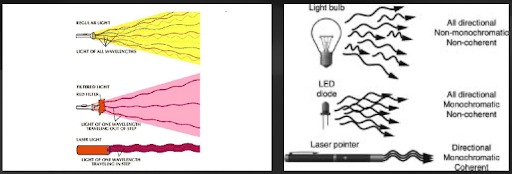
With LEDs, the light is also all-direction, but it comes out in a single wavelength that is monochromatic, but it is still non-coherent, travelling in varying directions. Laser, on the other hand, is the only option that has directionality, is monochromatic, and is coherent, so all of those monochromatic photons are travelling in the exact same direction, exactly where it is applied by the practitioner.
The differences in these actions (and therefore their therapeutic outcomes) is exactly why a 2017 study [15] concluded that NON-laser light sources (lamps with or without filters, LEDs with or without a polariser, etc) cannot be used in low-level laser therapy because of their minimal efficiency. Obviously, LEDs have their niche in a vast field of light therapy, for example, they are very successfully used in photodynamic therapy, and UV LEDs have a good bactericidal effect, but to expect clinical effects similar to those obtained precisely in low-level laser therapy using laser light (LLLT) from them may be a waste of time. Laser therapy – as the name suggests, should only be conducted with lasers and no other light sources.
Laser vs LEDs
To better understand the difference between laser and LEDs, we think of the principles of directionality and coherence that we mentioned above. Having an LED light positioned above your head may be having a therapeutic effect to a certain limited extent, but because the light being produced is not monochromatic or coherent, it’s not going to have nearly as good absorption.
As confirmed by a study [16], the illumination of the investigated molecules directly with the laser light, and with the light of the incandescent lamp through light filters showed that the illumination from the laser is absorbed several times more actively than incoherent light with a larger spectral width – so laser light is absorbed more actively, so it’s going to have a better photochemical effect.
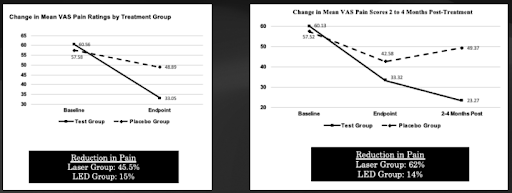
Erchonia have then gone on to prove their effects as part of their FDA clearance across their pain studies that include 5 double-blind studies. These studies compared the 635 nm laser (indicated by the solid black line) to a 635 nm LED (indicated by the dashed line) – and you can see the results are significant, showing that LED works – but not nearly as well as the laser. Interestingly, laser therapy maintained its therapeutic effects after the laser treatment ended, whereas the LED group regressed and pain increased somewhat.
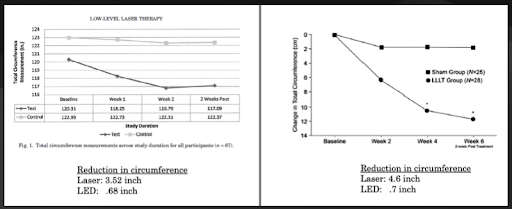
Erchonia has achieved the same results for laser applications outside the EVRL, such as their Emerald laser for body fat circumference reduction. With the application of the same wavelength of laser vs LED, they showed that laser was able to achieve six times better results than LED, as pictured below.
Class IV Lasers
When we look at the FDA clearance of class IV lasers, they are cleared under the ILY product code. This category on the FDA website started as a heating pad, and expanded to thermal lasers that are intended to “provide topical heating for the purpose of elevating tissue temperature for temporary relief of muscle and joint pain and stiffness, arthritis pain, or muscle spasm, the temporary increase in local blood circulation and/or promoting relaxation of muscle”. The FDA has now made the ILY products 510(k) exempt based on the device requirements of raising skin temperature to 40-45°C.
This mechanism of action now makes sense – most class IV lasers are using infrared, and that infrared wavelength is being absorbed by water molecules which creates a vibrational rotational effect that leads to the photothermal effect, leading to the heating we feel.
Simply put, in order for the FDA to clear a class IV laser and give a device that classification, it only needs to prove that it can raise the skin temperature to 40-45 degrees – ticking the boxes for it to be a topical heating product – which ironically can also be achieved by an infrared heat lamp.
Unfortunately, the rise in temperature creates a concern as most proteins, DNA, RNA, membranes and their integral structures start to unwind or melt at temperatures ranging from 40-100°C, with the result being denaturation or loss of function of the molecular structures [17]. These effects, accompanied by bond destruction and membrane alterations are summarised in the single term, hyperthermia, ranging from approximately 42-50°C. If such hyperthermia lasts for several minutes, a significant percentage of the tissue will already undergo necrosis.
Additionally, studies have established that free radicals are produced during IR irradiation of human skin [18]. This effect was demonstrated in vivo by resonance Raman spectroscopy (RRS) measurements and confirmed by electron paramagnetic resonance (EPR) spectroscopic investigations. Heating to ~41°C, free radical formation was almost doubled, and antioxidant power was reduced to about 50%.
Have any questions about the information presented in this article, the EVRL laser, its therapeutic effects, or getting started with the EVRL laser in your clinic? Contact Rehacare on 1300 653 522.
- [1]: Chung H, Dai T, Sharma SK, Huang Y-Y, Carroll JD, Hamblin MR. The Nuts and Bolts of Low-level Laser (Light) Therapy. Ann Biomed Eng. 2012;40(2):516–33.
- [2]: Hamblin MR, Demidova TN. Mechanisms of low level light therapy. Mech Low-light Ther. 2006;614001-614001–12.
- [3]: Huang YY, Chen AC, Carroll JD, Hamblin MR. Biphasic dose response in low level light therapy. Dose- response. 2009 Oct 1;7(4):dose-response.
- [4]: Pereira AN, Eduardo CD, Matson E, Marques MM. Effect of low‐power laser irradiation on cell growth and procollagen synthesis of cultured fibroblasts. Lasers in Surgery and Medicine: The Official Journal of the American Society for Laser Medicine and Surgery. 2002 Oct;31(4):263-7.
- [5]: Sommer AP, Pinheiro AL, Mester AR, Franke RP, Whelan HT. Biostimulatory windows in low-intensity laser activation: lasers, scanners, and NASA’s light-emitting diode array system. Journal of clinical laser medicine & surgery. 2001 Feb 1;19(1):29-33.
- [6]: Sutherland JC. Biological Effects of Polychromatic Light. Photochemistry and photobiology. 2002 Aug;76(2):164-70.
- [7]: ARPANSA. Lasers [homepage on the Internet]. Commonwealth of Australia: Australian Radiation Protection and Nuclear Safety Agency; {cited 2022 Jul 25]. Available from: https://www.arpansa.gov.au/ understanding-radiation/what-is-radiation/non-ionising-radiation/laser
- [8]: Huang YY, Chen AC, Carroll JD, Hamblin MR. Biphasic dose response in low level light therapy. Dose- response. 2009 Oct 1;7(4):dose-response.
- [9]: Hamblin MR, Demidova TN. Mechanisms of low level light therapy. Mech Low-light Ther. 2006;614001-614001–12.
- [10]: Huang YY, Chen AC, Carroll JD, Hamblin MR. Biphasic dose response in low level light therapy. Dose- response. 2009 Oct 1;7(4):dose-response
- [11]: Silverman RG, Comey A, Sammons T. Effects of a single treatment with two nonthermal laser wavelengths on chronic neck and shoulder pain. Medical Devices Auckl N Z. 2019;12:319–25.
- [12]: Roche GC, Murphy DJ, Berry TS, Shanks S. Low-Level Laser Therapy for the Treatment of Chronic Neck and Shoulder Pain. Funct Neurol Rehabil Ergon. 2016;6(2):97–104.
- [13]: Silverman RG, Comey A, Sammons T. Effects of a single treatment with two nonthermal laser wavelengths on chronic neck and shoulder pain. Medical Devices Auckl N Z. 2019;12:319–25.
- [14]: Tomazoni SS, Almeida MO, Bjordal JM, Stausholm MB, Machado C dos SM, Leal-Junior ECP, et al. Photobiomodulation therapy does not decrease pain and disability in people with non-specific low back pain: a systematic review. J Physiother. 2020;66(3):155–65.
- [15]: Moskvin SV. Only lasers can be used for low level laser therapy. Biomedicine. 2017;7(4):22
- [16]: Dubrovskiĭ VA, Gusev VV, Astaf’eva OG. O roli fizicheskikh kharakteristik lazernogo izlucheniia v pogloshchenii sveta gemosoderzhashchimi biologicheskimi molekulami [Role of physical properties of laser radiation in light absorption by heme-containing biological molecules]. Biofizika. 1982 Sep-Oct;27(5):908-9. Russian. PMID: 7138946.
- [17]: Jawad MM, Qade STA, Zaidan AA, Zaidan BB, Naji AW, Qade ITA. An Overview of Laser Principle, Laser-Tissue Interaction Mechanisms and Laser Safety Precautions for Medical Laser Users. Int J Pharmacol. 2011;7(2):149–60.
- [18]: Darvin ME, Haag SF, Lademann J, Zastrow L, Sterry W, Meinke MC. Formation of Free Radicals in Human Skin during Irradiation with Infrared Light. J Invest Dermatol. 2010;130(2):629–31.